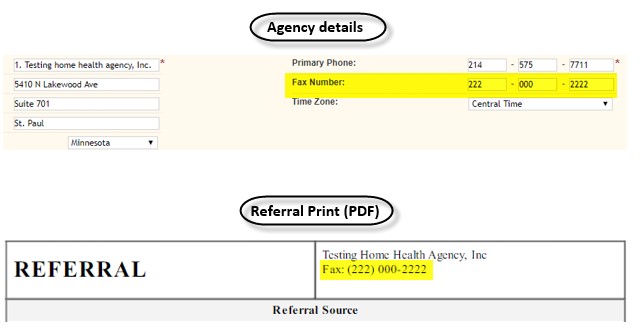
The agency’s fax number now populates on the print preview (PDF) of existing or a new referral (below the agency’s name).
Patient By Physician Listing
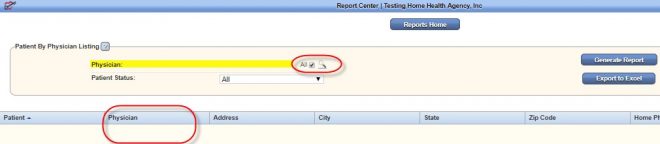
In the Report Center, the Patient By Physician Listing now has a new All check box for the physician field. If selected, the system will generate the specified patient status list for all physicians.
Note: When the All check box is selected, the physician’s search box will not be shown (since all physicians will be pulled as specified). A new Physician column is also now included in the listing.

Visits By Type
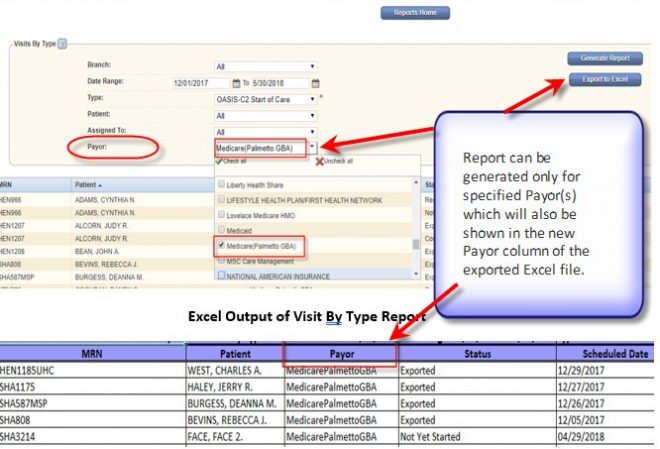
The Visits By Type report now has a new Payor filtering field. This allows users to select to run the report for specific or all payors. The exported Excel file will also have a new Payor column (between the Patient and Status columns) to show the payor name for the patient’s visiting date.
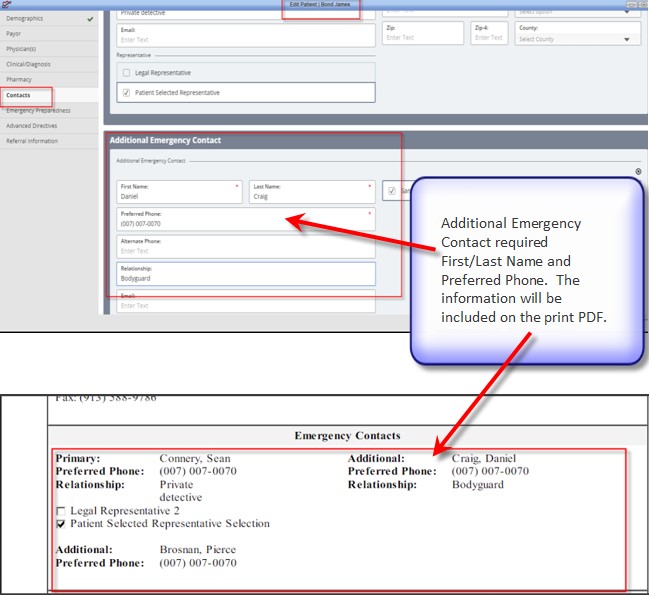
Additional Emergency Contact
The Additional Emergency Contact in the Edit Patient window is now being validated for the following required fields: First Name, Last Name, and Preferred Phone. Similar with the Primary Emergency Contact, the validation for Additional Emergency Contact will pass if all three required fields are either blank (empty) or have data. Otherwise, the validation fails and will not save.
Additional Emergency Contact will be shown on the print preview PDF next to the Primary Emergency Contact information.
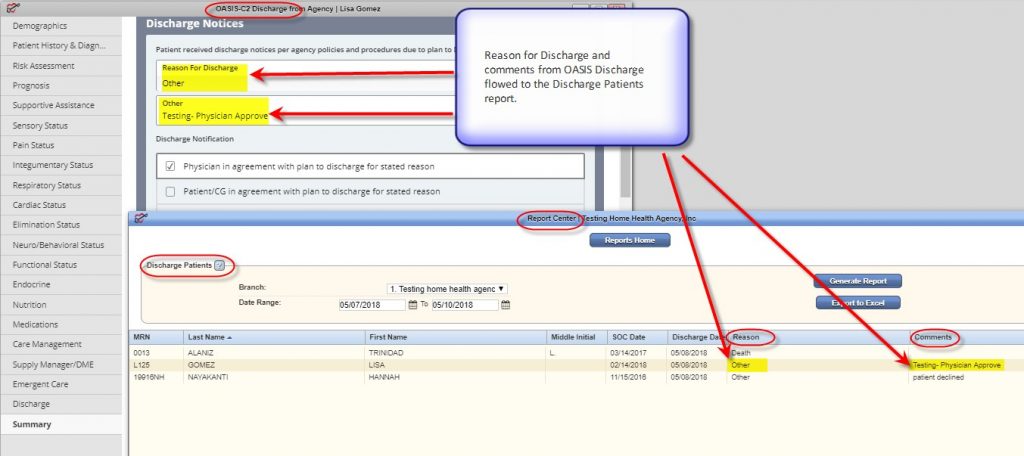
Reason for Discharge
The Reason for Discharge in the Summary tab of OASIS-C2 Discharge is now a single-select option. If the “Other” option is selected, a text box will be displayed allowing the clinician to enter the reason(s).
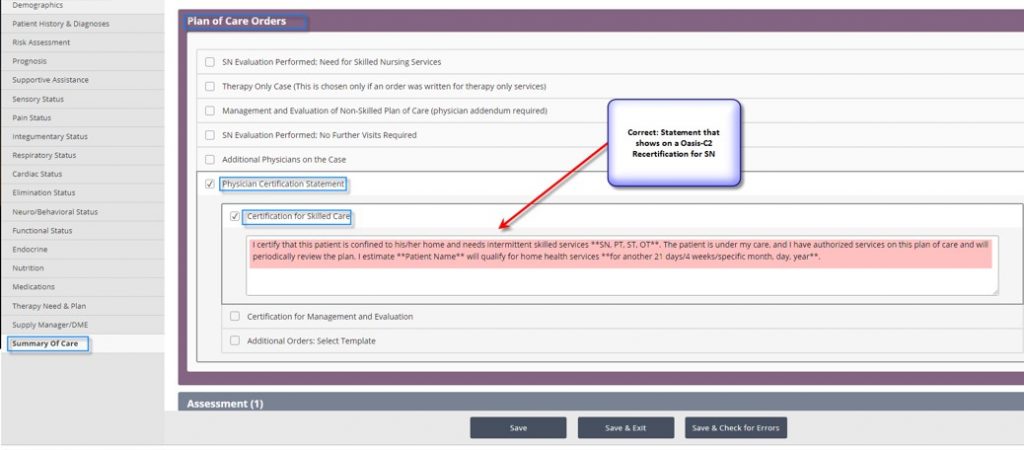
Certification for Skilled Care Statement
The Physician Certification for Skilled Care statement in OASIS-C2 (SN, PT, OT, ST) Recertification now displays as follows:
I certify that this patient is confined to his/her home and needs intermittent skilled services **SN, PT, ST, OT **. The patient is under my care, and I have authorized services on this plan of care and will periodically review the plan. I estimate **Patient Name ** will qualify for home health services **for another 21 days/4 weeks/specific month, day, year **.
Updated on 5/31/2018